There has been enough sporting competition over the summer to remind us how tough it can be to be the not-quite winner. In England, there was great excitement when the national football team made it to the final of the European championships, only to lose to Italy on penalties. There was an almost immediate backlash of racism and hatred towards the players who missed those crucial last shots on goal.
In the US Open tennis tournament, the women’s final was contested by two talented teenagers who had both done spectacularly well to get that far—but it was hard to witness the disappointment of the runner-up, Leylah Fernandez. And at the Tokyo Olympics, competitor after competitor told the cameras: ‘I’m not here for second place; I’m not here for silver.’
Yet in life, unlike in sport, surely second is good enough? We can’t all be winners but if we have a good education, a good job and all our material needs are met surely that suffices for our health and wellbeing?
To some extent this is true: nobody needs excessive income or wealth to be healthy and too big an income gap between rich and poor is damaging for population health and the good functioning of society. But it is also true that, just as in sport, being the not-quite winner does matter.
Social gradients
Almost all the major causes of death and disease have social gradients. They are not simply more common among the poor and those at the bottom of society while rare among the rest of the population. Instead, there is a steady gradient in the incidence of different diseases and causes of death between every rung on the social ladder. So, while morbidity and mortality are certainly highest among the worst off, if you are not quite at the top of the income bracket, not quite in the top social class or don’t have the most advanced possible education your risk of poor health, illness and death is still a little bit higher than for those just above you.
This is an almost ubiquitous pattern, all over the world. We see it in life expectancy and infant mortality, in health behaviours such as smoking and in obesity, chronic diseases, heart attacks, infections and most cancers. There are one or two exceptions, notably breast and prostate cancer, but otherwise social gradients in health are everywhere.
In the chart below, the bars show life expectancy for men and women in England, with the population divided into ten groups, from those living in the greatest deprivation on the left to those least deprived on the right. Usually, when we look at charts such as this, our attention is drawn to the differences between the top and the bottom—here there is a 9.5 year gap in life expectancy between the most and least deprived men, and 7.7 years between the most and least deprived women.
Life expectancy at birth by area deprivation deciles and sex, England 2018
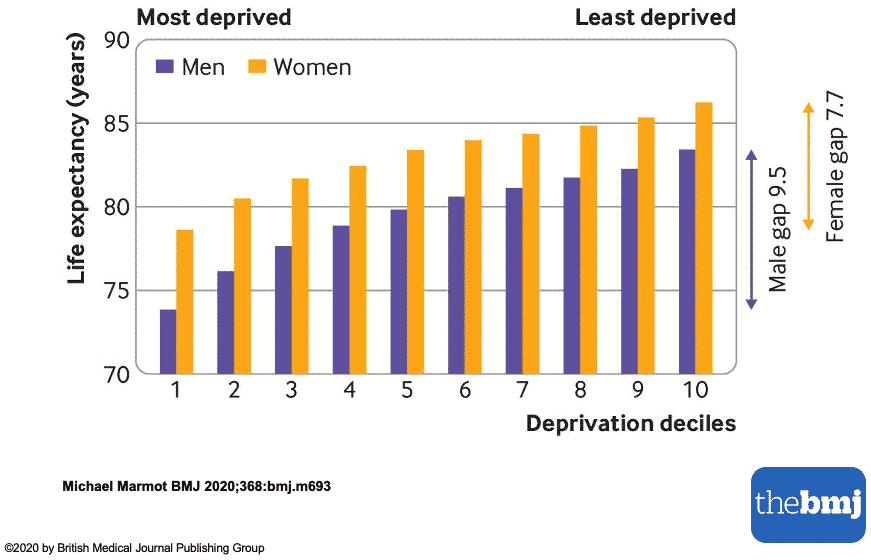
But at every step down from affluence to deprivation, from right to left, both men and women lose, on average, a little bit of life expectancy. Men in the second least deprived group are living on average about 82 years, about a year and a half less than men in the least deprived group of all. Women in the second to top group live just over 85 years but women in the very top group live about a year longer.
Those are surprising penalties for being among the not-quite least deprived rather than making it into the top 10 per cent. Nobody in the top 20 per cent is denied any material necessity and none is likely to lack the knowledge to make healthy choices. Yet those in the second decile still die younger and suffer higher rates of almost every acute or chronic illness than those in the first.
Status matters
What these social gradients tell us is how important the social environment is—it’s status itself that matters. If you have a little bit less status than those at the top, you don’t do as well as if you have the highest status. If we want to tackle inequalities in health, we have to flatten the whole gradient, not just try to tackle health problems at the bottom.
While social gradients in health are near-ubiquitous, the steepness of the gradient varies from place to place. There is a widespread tendency for societies with smaller economic inequalities to have smaller absolute differences in health. Reducing inequalities in income, wealth, education and social class will help the whole of society—not just the poorest or those living in the deepest deprivation. We would all be winners if the playing-field were levelled.
Covid-19 has a social gradient too, of course. It was never an ‘equal-opportunity disease’, as some suggested early on. It’s too late for the pandemic we’re in, but some serious social and economic levelling would help us cope with whatever might come next.
This is a joint publication by Social Europe and IPS-Journal
